Connect With BioMarin
Register to get Brineura updates, as well as helpful resources and information.
The safety of Brineura® (cerliponase alfa) was evaluated in 24 patients with CLN2 disease who received at least 1 dose of Brineura in a clinical study with extension of up to 161 weeks.1
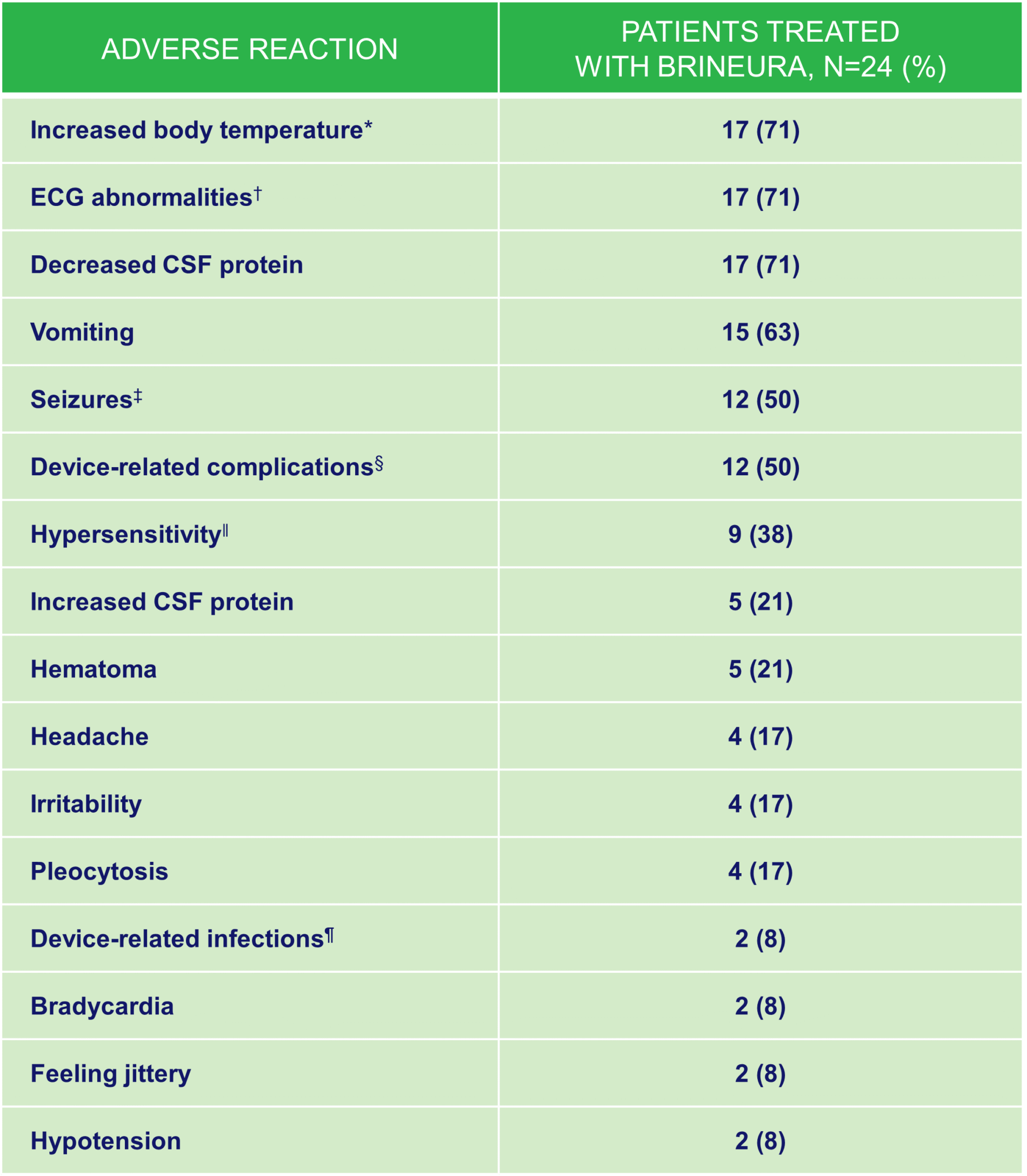
*Increased body temperature includes: increased body temperature and pyrexia.
†ECG abnormalities include: non-specific repolarization abnormality, notched QRS, ST segment elevation, biphasic T wave abnormality, supraventricular extrasystoles,bradycardia, sinus tachycardia, and intraventricular conduction delay.
‡Seizures include: atonic, generalized tonic-clonic, focal, and absence.
§Device-related complications include device-related infection, delivery system-related complications (needle issues, device leakage, device malfunction, device difficult to use, medical device site irritation, device breakage, etc) and pleocytosis.
||Hypersensitivity includes only hypersensitivity.
¶Device-related infections include: Propionibacterium acnes and Staphylococcus epidermidis.
The most frequent adverse reactions reported in patients <3 years treated with Brineura were similar to those observed in patients ≥3 years of age except for hypersensitivity reactions, which were reported in 5 of 8 (63%) patients <3 years at baseline compared with 0 of 6 in patients ≥3 years of age at baseline. The most common manifestations of hypersensitivity were pyrexia and vomiting and the timing and resolution were similar to Trials 1 and 2.1
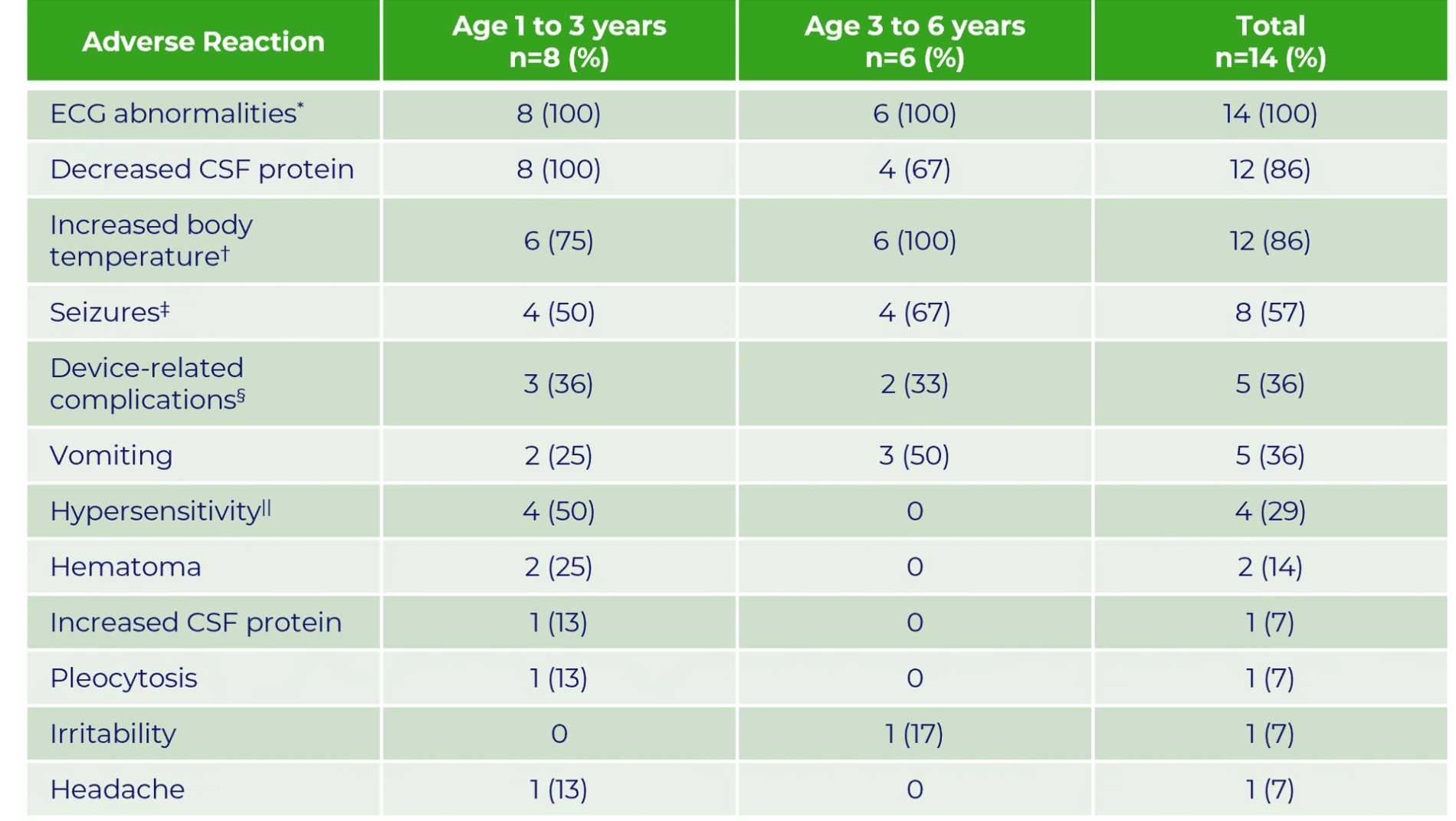
Note: Incidence numbers are based on baseline age group.
*ECG abnormalities include: non-specific repolarization abnormality, supraventricular extrasystoles, possible left ventricular hypertrophy, intermittent 2nd degree AV Block (type 2 Mobitz), incomplete right bundle branch block, and prominent Q wave.
†Increased body temperature includes: increased body temperature and pyrexia.
‡Seizures include: atonic, febrile convulsion, generalized tonic-clonic, partial, partial with secondary generalization, petit mal epilepsy, myoclonic and status epilepticus.
§Device-related complications include device-related infection, delivery system-related complications (needle issues, device leakage, device malfunction, device difficult to use, medical device site irritation, device breakage, etc).
||Hypersensitivity includes only the term of hypersensitivity.
• In Trial 3, infusion-associated reactions were reported in 8 of 8 patients less than 3 years of age at baseline as compared with 4 of 6 patients ≥3 years of age at baseline
ECG, electrocardiogram.
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in practice.
Due to the potential for anaphylaxis, appropriate medical support should be readily available including access to cardiopulmonary resuscitation equipment, and patients should be observed closely, during and after Brineura infusion. If anaphylaxis occurs, immediately discontinue infusion and initiate appropriate medical treatment. Inform patients/caregivers of the signs and symptoms of anaphylaxis and to seek immediate medical care should these occur. Consider the risks and benefits of readministration of Brineura following an anaphylactic reaction.
To report suspected adverse reactions, contact:
BioMarin Pharmaceutical Inc.
Phone: 1-866-906-6100
Email: drugsafety@bmrn.com
FDA
Phone: 1-800-FDA-1088
Web: www.fda.gov/medwatch
For medical information inquiries:
BioMarin Medical department
Email: medinfo@bmrn.com
Phone: 1-800-983-4587
WARNING: HYPERSENSITIVITY REACTIONS INCLUDING ANAPHYLAXIS
Patients treated with enzyme replacement therapies have experienced life-threatening hypersensitivity reactions, including anaphylaxis. These reactions have occurred during and up to 24 hours after completion of the Brineura infusion. Anaphylaxis has occurred during the early course of enzyme replacement therapy and after extended duration of therapy.
Administration of Brineura should be supervised by a healthcare provider knowledgeable in the management of hypersensitivity reactions including anaphylaxis. Initiate Brineura in a healthcare setting with appropriate medical monitoring and support measures, including access to cardiopulmonary resuscitation equipment. If a severe hypersensitivity reaction (e.g., anaphylaxis) occurs, discontinue Brineura and immediately initiate appropriate medical treatment, including use of epinephrine. Inform patients of the symptoms of life-threatening hypersensitivity reactions, including anaphylaxis and to seek immediate medical care should symptoms occur.
Patients less than 3 years of age may be at increased risk for developing hypersensitivity reactions with Brineura use compared to patients 3 years of age and older.
Observe patients closely during and after the infusion. The management of hypersensitivity reactions should be based on the severity of the reaction and may include temporarily interrupting the infusion, and/or treatment with antihistamines, antipyretics, and/or corticosteroids. Consider the risks and benefits of readministration of Brineura following an anaphylactic reaction. If the decision is made to readminister Brineura after the occurrence of anaphylaxis, ensure appropriately trained personnel and equipment for emergency resuscitation (including epinephrine and other emergency medicines) are readily available during infusion. Initiate subsequent infusion at approximately one‑half the initial infusion rate at which the anaphylactic reaction occurred.
Contraindications
Brineura is contraindicated in patients with:
Recommendations Prior to Brineura Treatment
Premedication of patients with antihistamines with or without antipyretics or corticosteroids is recommended 30-60 minutes prior to the start of infusion. Brineura must only be administered via the intraventricular route using aseptic technique to reduce the risk of infection. Administer Brineura and the Intraventricular Electrolytes using the provided Administration Kit for use with Brineura components. Prior to each infusion, inspect the scalp for signs of intraventricular access device leakage or failure and for potential infection. Prior to each infusion of Brineura and when clinically indicated, send cerebrospinal fluid (CSF) samples for testing of cell count and culture. Replace the intraventricular access device reservoir prior to 4 years of single-puncture administrations.
Special Populations
Brineura is not recommended in patients less than 37 weeks post‑menstrual age (gestational age at birth plus post‑natal age) or those weighing less than 2.5 kg.
Brineura has not been studied in pregnancy or lactation
WARNINGS AND PRECAUTIONS
Meningitis and Other Intraventricular Access Device-Related Infections
Bacterial meningitis requiring antibiotic treatment and removal of the device was reported during postmarketing use of Brineura. The signs and symptoms of infections may not be readily apparent in patients with CLN2 disease. To reduce the risk of infectious complications, Brineura should be administered by, or under the supervision of, a physician experienced in intraventricular administration.
Intraventricular Access Device-Related Complications
During the clinical trials and in postmarketing reports, intraventricular access device-related complications were reported (e.g., device leakage, device failure, extravasation of CSF fluid, or bulging of the scalp around or above the intraventricular access device). In case of intraventricular access device-related complications, discontinue the Brineura infusion and refer to the device manufacturer’s labeling for further instructions.
Material degradation of the intraventricular access device reservoir was reported after approximately 4 years of administration, which may impact the effective and safe use of the device. The intraventricular access device should be replaced prior to 4 years of single-puncture administrations, which equates to approximately 105 administrations of Brineura.
Cardiovascular Adverse Reactions
Monitor vital signs before infusion starts, periodically during infusion, and post-infusion in a healthcare setting. Perform electrocardiogram (ECG) monitoring during infusion in patients with a history of bradycardia, conduction disorder, or with structural heart disease. In patients without cardiac abnormalities, regular 12-lead ECG evaluations should be performed every 6 months.
Infusion Associated Reactions (IAR) such as vomiting, seizure, rash, pyrexia, hypersensitivity, and anaphylactic reaction have been observed in patients treated with Brineura. If an IAR occurs, decreasing the infusion rate, temporarily stopping the infusion, and/or administering antihistamines and/or antipyretics may ameliorate the symptoms. Closely monitor patients who have experienced IARs when re-administering Brineura.
ADVERSE REACTIONS
In clinical trials, the most frequently reported adverse reactions (≥8%) were pyrexia, ECG abnormalities, decreased CSF protein, vomiting, seizures, device-related complications, hypersensitivity, increased CSF protein, hematoma, headache, irritability, pleocytosis, device-related infection, bradycardia, feeling jittery, and hypotension. The most frequent adverse reactions reported in patients < 3 years of age treated with Brineura were similar to those observed in patients > 3 years of age except for hypersensitivity reactions, which were reported in 5 of 8 (63%) in patients < 3 years of age at baseline compared with 0 of 6 in patients > 3 years of age at baseline. The most common manifestations of hypersensitivity were fever and vomiting. Such symptoms resolved over time or with administration of antipyretics, antihistamines and/or corticosteroids.
To report SUSPECTED ADVERSE REACTIONS, contact BioMarin Pharmaceutical Inc. at 1-866-906-6100, or FDA at 1-800-FDA-1088, or go to www.fda.gov/medwatch.
Please see accompanying full Prescribing Information, with Boxed Warning for risk of anaphylaxis or visit www.Brineura.com.
INDICATION
Brineura (cerliponase alfa) injection for intraventricular use is indicated to slow the loss of ambulation in pediatric patients with neuronal ceroid lipofuscinosis type 2 (CLN2 disease), also known as tripeptidyl peptidase 1 (TPP1) deficiency.